
British Asians are underrepresented in clinical studies.
‘When British Asians are excluded from clinical research, Asian communities remain overlooked in cancer prevention, access to care, diagnosis, and innovative treatments. Care is less tailored and outcomes are poorer.‘
This lack of inclusion and representation means that British Asians live less well with cancer and die sooner than other people. Researchers are keen to address this.
This inequity is a major patient safety issue, which the British Asian Cancer Charity is focusing on through the BACC research focus group, which forms part of the #MyResearchLegacy campaign.
We believe that one of the most powerful ways to recruit people from underrepresented groups to clinical studies is by word of mouth and by sharing information through networking.
Opportunities to be part of research projects:
Here are details of academic research projects which relate to British Asians with cancer. Please share these with colleagues, friends, relatives and anyone who may be interested.
- The REFORM study – a study working with South Asian women to explore their experiences of breast cancer and hormone therapy to understand how to improve support for South Asian women and reduce ethnic health inequalities.
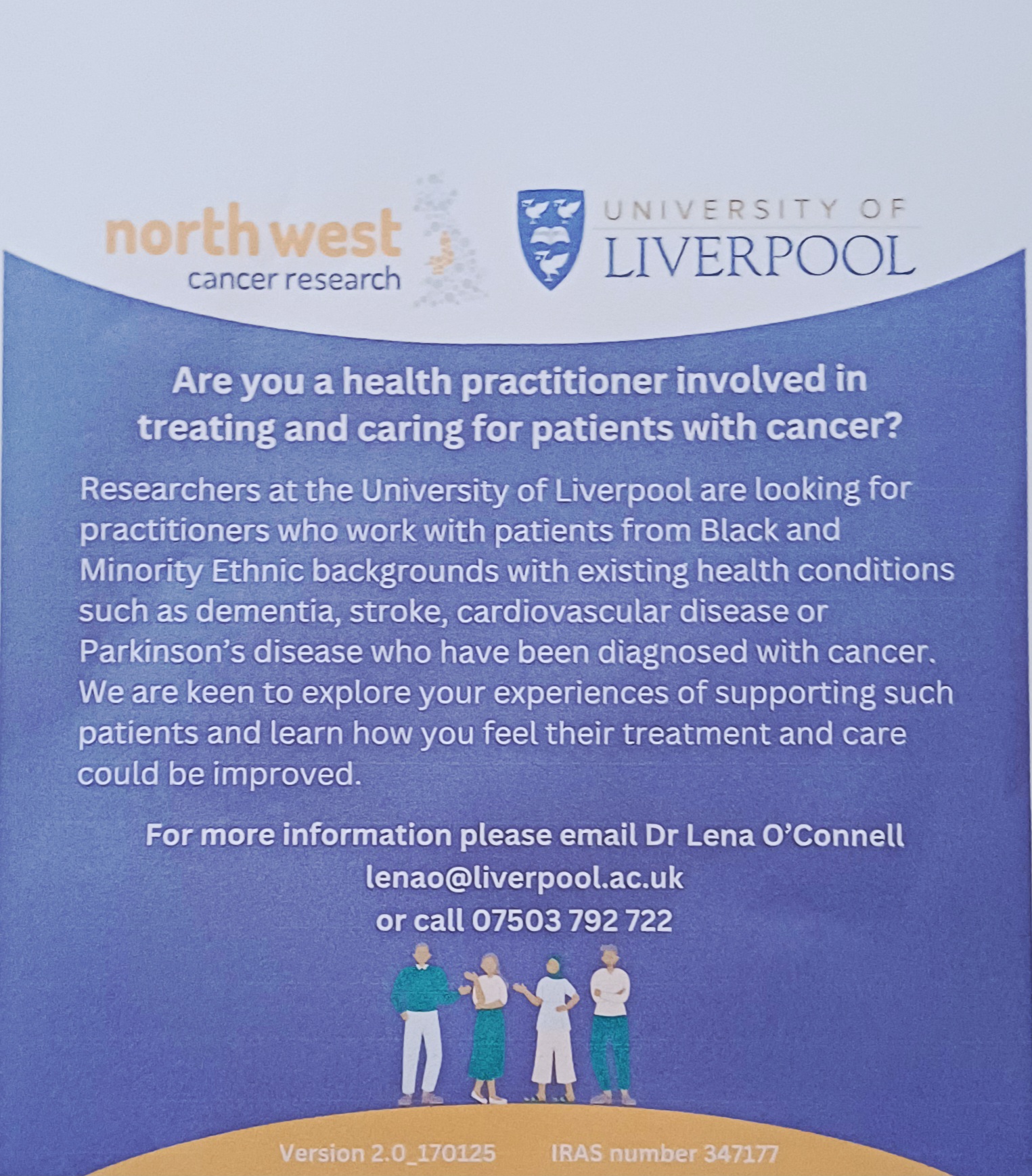
- The UNITY study – which is recruiting healthcare practitioners who work with people who have cancer and another serious illnesses(s) to learn how treatment and care can be improved.
- The SEARCH study – which is looking for patients to help design a study which aims to improve early detection on lung cancer in people who have been treated for Hodgkin Lymphoma.
- The SPARK study – which is comparing cancer patients recruited by hospitals with those recruited by patient organisations. The aim of this project is to guide future research and guideline development to improve the quality and efficiency of recruitment strategies.
Posters:
The REFORM study – recruiting South Asian women. Aim of this study – to understand how to improve support for South Asian women and reduce ethnic health inequalities.
The UNITY study – recruiting healthcare practitioners. Aim of this study – to learn how treatment and care can be improved.
The SEARCH study – recruiting Hodgkin Lymphoma survivors. Aim of this study – to improve early detection on lung cancer in people who have been treated for Hodgkin Lymphoma.
The SPARK study – which is recruiting cancer patients (all types of cancer). Aim of this study – to guide future research and guideline development to improve the quality and efficiency of recruitment strategies.
This blog was produced on behalf of the British Asian Cancer Charity Research Focus Group. This group is open to everyone, clinicians, patients, relatives, carers.
The group’s objectives are:
- Promoting Research Initiatives: Actively supporting and following up on research that directly benefits British Asians affected by cancer.
- Identifying Gaps and Opportunities: Pinpointing areas where current data is insufficient and highlighting new avenues for impactful research.
- Driving Measurable Improvement: Advocating for and implementing evidence-based changes in cancer care.
Click here to receive the BACC research focus group emails Your details will not be shared with third parties, you can unsubscribe at any time (no questions asked), and you will not receive spam.
To find out more about The British Asian Cancer Charity click here: https://linktr.ee/BritAsianCancer
Author: Steve Turner – Chair of the British Asian Cancer Charity. Charity Commission Reg. no 1212093 – Data Protection Reg no: ZC044416 For more information contact: steve@cancerequity.org.uk
British Asian Cancer Charity www.cancerequity.org.uk Research Focus Group Newsletter:1 Version:1 29.02.2026












{kind=link}