British Asians are underrepresented in clinical studies.
‘When British Asians are excluded from clinical research, Asian communities remain overlooked in cancer prevention, access to care, diagnosis, and innovative treatments. Care is less tailored and outcomes are poorer.‘
This lack of inclusion and representation means that British Asians live less well with cancer and die sooner than other people. Researchers are keen to address this.
This inequity is a major patient safety issue, which the British Asian Cancer Charity is focusing on through the BACC research focus group, which forms part of the #MyResearchLegacy campaign.
We believe that one of the most powerful ways to recruit people from underrepresented groups to clinical studies is by word of mouth and by sharing information through networking.
Opportunities to be part of research projects:
Here are details of academic research projects which relate to British Asians with cancer. Please share these with colleagues, friends, relatives and anyone who may be interested.
The REFORM study – a study working with South Asian women to explore their experiences of breast cancer and hormone therapy to understand how to improve support for South Asian women and reduce ethnic health inequalities.
The UNITY study – which is recruiting healthcare practitioners who work with people who have cancer and another serious illnesses(s) to learn how treatment and care can be improved.
The SEARCH study – which is looking for patients to help design a study which aims to improve early detection on lung cancer in people who have been treated for Hodgkin Lymphoma.
The SPARK study – which is comparing cancer patients recruited by hospitals with those recruited by patient organisations. The aim of this project is to guide future research and guideline development to improve the quality and efficiency of recruitment strategies.
This blog was produced on behalf of the British Asian Cancer Charity Research Focus Group. This group is open to everyone, clinicians, patients, relatives, carers.
The group’s objectives are:
Promoting Research Initiatives: Actively supporting and following up on research that directly benefits British Asians affected by cancer.
Identifying Gaps and Opportunities: Pinpointing areas where current data is insufficient and highlighting new avenues for impactful research.
Driving Measurable Improvement: Advocating for and implementing evidence-based changes in cancer care.
Author: Steve Turner – Chair of the British Asian Cancer Charity. Charity Commission Reg. no 1212093 – Data Protection Reg no: ZC044416 For more information contact: steve@cancerequity.org.uk
British Asian Cancer Charity www.cancerequity.org.uk Research Focus Group Newsletter:1 Version:1 29.02.2026
The Protection for Whistleblowing Bill [HL]1 which passed its second reading in December 2022, proposes the repeal of the current Public Interest Disclosure Act2 [PIDA], replacing it with an Office of the Whistleblower [OWB]. This would prevent concerns of genuine healthcare whistleblowers becoming buried under an employment issue, and their original issues being sidelined. There are many examples of this happening, the most recent being the treatment of whistleblowers who raised concerns over a nurse who was later found guilty of murdering seven babies and attempting to murder another six3. Because the people who first raised concerns were initially bullied and intimidated into silence, it was a year before the initial concerns were acted upon, during which time the nurse went on to murder a further 5 babies and attempt to murder a further five4.
Why do we need a change in the law?
Current UK whistleblowing law, the Public Interest Disclosure Act2 [PIDA], is expensive, limited in scope and beyond the reach of most whistleblowers. It is also overly complex, with cases currently waiting for over 2 years to be heard. Employers game the system to run whistleblowers out of funds.
PIDA does not protect patients and is not accessible to members of the public who blow the whistle. Currently there is no statutory provision to investigate or address the wrongdoing highlighted by whistleblowers, and whistleblowers have been denied any protection because they are not workers.
Media reports on whistleblowing in healthcare tend to focus our attention on senior people and on Employment Tribunals. Behind every high-profile whistleblower in health and social care there are many more people who are suffering detriment for speaking out and have not been able, or not wanted, to take legal action. This includes people at all levels in the organisations and from all professions. This is a drain on the resources of our health system as many take early retirement, change careers, or emigrate to remove themselves from the situation.
Sadly, when staff are unable to speak out or are silenced it falls on patients and their relatives to do this. They effectively become whistleblowers, without any legal protection.
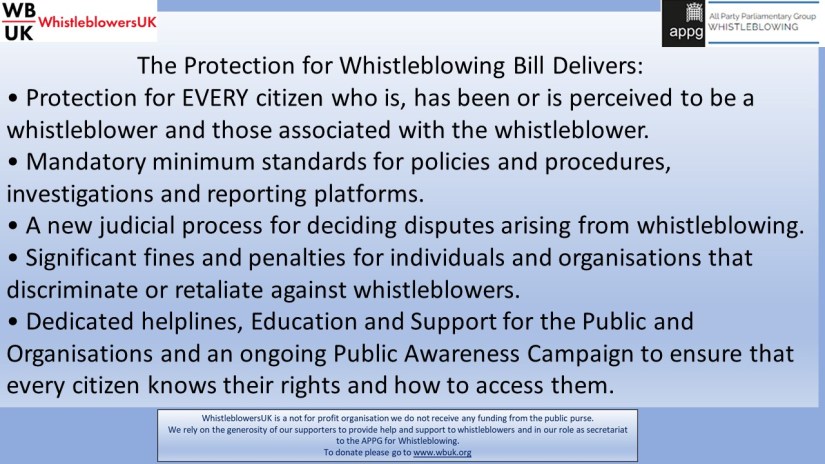
The Protection for Whistleblowing Bill replaces PIDA and introduces an Office of the Whistleblower. This will change the landscape and help us identify root causes of systemic patient safety failings. This has the potential to save lives, halt corruption, and safeguard people who speak out.
I urge everyone with an interest to read the Bill itself and decide on your position based on the facts.
NO. The OWB will support the work of the Ombudsman by identifying themes and areas of concerns, and by setting standards for investigations.
2. Will the Office of the Whistleblower be ‘another regulator’?
NO. The OWB will provide independent scrutiny of whistleblowing which will help support the work of regulators and bring together the various ‘speak up’ initiatives that are in place.
3. Which whistleblowers will be protected by the Office of the Whistleblower [OWB]?
The OWB will protect all citizens, putting an end to the limitations and restriction set out in PIDA which limits who can be helped and who is protected. Under PIDA protection afforded is only in respect of breaches of contract between employer and employee. This approach doesn’t represent the realities of the modern world and the complexities of areas such as healthcare where the customers / patients / users of services have a key role in shared decision making.
4. Will the Office of the Whistleblower only focus on high profile cases and senior people?
NO. The OWB will be available to all citizens. Currently many whistleblowers are denied protection because they are not workers. These include families like those at Gosport Memorial Hospital, residents of Grenfell Tower, and the families of victims of Maternity failings.
5. What will happen to whistleblower who were / are being protected by the Public Interest Disclosure Act when it is scrapped?
There will be a planned transition to ensure nobody is disadvantaged by the repeal of PIDA.
6. Wouldn’t it be simpler, and just as effective, to amend PIDA?
NO. Whistleblowing is not an employment issue!
Employment Tribunals cannot take action or make decisions about the merits of a protected disclosure and even if they could there are serious consequences for the public interest.
PIDA is unamendable. PIDA is expensive, limited in scope and beyond the reach of most whistleblowers. It is also overly complex, with cases currently waiting for over 2 years to be heard. As a result, employers can (and do) game the system by exhausting and running whistleblowers out of funds.
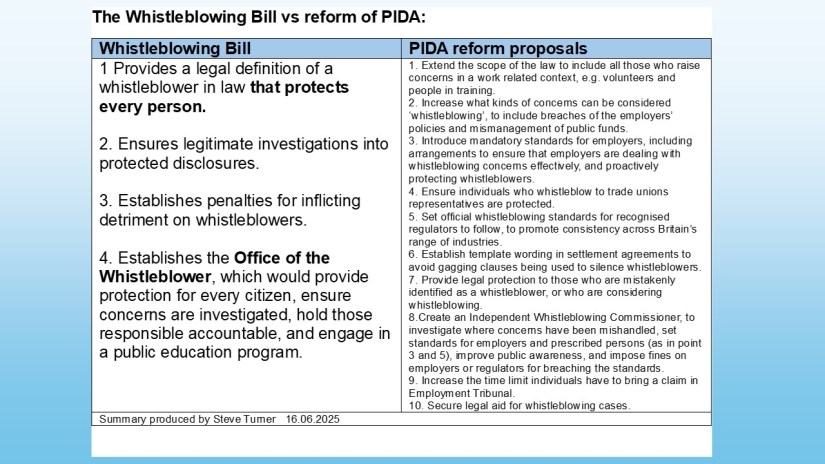
The Whistleblowing Bill tackles the root causes of the problems. It’s more inclusive, simple and clear. As shown in this comparison:
7. Are the measures in the Protection for Whistleblowing Bill based on the US ‘bounty hunting’ model of rewards for whistleblowers? No.
The Bill was informed by evidence from the UK and around the world. This includes whistleblowers themselves as experts by experience.
8. What is meant by ‘restitution’ for whistleblowers?
The word restitution means the restoration of something to its original state. This most accurately describes what the Office of the Whistleblower will aim to achieve. The objective is restoration of whistleblowers to the state they were in, or would have been in, had it not been for the fact they had to blow the whistle on wrongdoing.
There will be additional ways to recognise whistleblowers as part of the drive to normalise speaking up. Talk of rewards, bounty and compensation has dominated the negative narrative against change and does not reflect the real objective of Office of the Whistleblower, provision of a robust and comprehensive response to detriment imposed on whistleblowers.
9. Will the Bill and Office of the Whistleblower open the floodgates to people with a grudge and to spurious claims?
NO. The Bill includes checks and balances to be fair to all parties and contains a provision to exclude frivolous, malicious or vexatious whistleblowing claims.
10. Will the Protection for Whistleblowing Bill end the practice of ‘gagging’ whistleblowers through non-disclosure agreements [NDAs]?
YES. It is an important and integral part of the Bill that will address the practice of suppressing whistleblowing.
N.B. the new law will improve compliance that has so far been absent.
11. How will the Office of the Whistleblower be funded?
The Office of the Whistleblower will be set up by the Secretary of State and initially funded by government. As time progresses the Office will become self-sufficient, being funded by fines imposed on organisations that fail to be compliant.
The Office of the Whistleblower will not receive sponsorship funding or be linked to specific organisations in a way that compromises its integrity.
12. Does the Bill define whistleblowing?
YES. One of the major failings of PIDA was the failure to use simple terms that everyone understands including defining whistleblowing and whistleblowers in law. This has watered down workers’ rights in an already ineffective law and left the rest of the public unprotected.
13. Under the Bill can people still make a protected disclosure, and who will the ‘prescribed persons’ be?
YES. To support this, the definition of ‘prescribed persons’ is changed to ‘relevant person’. This removes the constraints set out in PIDA which cause confusion and are used by employers to game the system.
14. How will the independence of the Office of the Whistleblower be maintained and monitored?
Accountability for the Office of the Whistleblower rests with the Secretary of State, who is accountable to Parliament, and to the electorate.
Section 5 of the Bill sets out the governance arrangements.
16. Will the Office of the Whistleblower replace Employment Tribunals?
NO. The OWB will be specifically for whistleblowing to ensure that public safety matters and retaliation are dealt with by an organisation that is properly equipt to do so. The OWB will put an end to inappropriate, and hugely expensive, use of Employment Tribunals to address whistleblowing concerns, (other employment matters including pay and discrimination will remain the jurisdiction of the ET).
17. What powers will the Office of the Whistleblower have?
The Office of the Whistleblower will have teeth. This includes powers to issue information notices and action notices, will have the power to impose civil and refer criminal offenses.
18. Can people appeal against the decisions of the Office of The Whistleblower?
19. Why do we need another organisation for whistleblowers?
We don’t, The Office of the Whistleblower is a new type of body that provides independent oversight of whistleblowing and does not duplicate the work of other bodies. The overall aim of the OWB is to ensure that the public interest is protected. The work of the OWB will enhance and support all existing organisations including regulators and law enforcement.
20. What happens if whistleblowers cannot afford to pursue their case?
The OWB is a free service and will adjudicate on issues of retaliation and detriment. The Bill sets out additional support for workers who can claim ‘interim relief orders’ to offset immediate financial or other hardship.
Part 11 of the Bill sets out the process for first and second tier appeals tribunals.
21. How will an Office of the Whistleblower cope with the inevitable deluge of requests for help, without becoming overwhelmed?
‘The strength of the Office of The Whistleblower [OWB] lies in its ability to formally request information, commission investigations, mandate action and set standards. For the first time, the Protection for Whistleblowing Bill defines whistleblowing and includes statutory powers. The Bill introduces civil penalties for whistleblower victimisation and a new criminal offence for any person who intentionally or recklessly submits a person to detriment.
The Office of the Whistleblower is a new type of body that provides independent oversight of whistleblowing. This will help unearth the root causes of whistleblower victimisation and drive forward actions to prevent a recurrence.
The inevitable deluge of requests for help will be welcome. For the first time, these can be investigated scrupulously and effectively. Accountability will be highlighted, and lack of accountability called out publicly. This will be backed up by the development of core principles and standards for effective education and learning.
The strength of the Office the Whistleblower is that it will not be a regulator, and not replace existing successful initiatives or organisations. The work of the OWB will support them. When it comes to healthcare, patient safety will be the focus, and the inappropriate use of employment law to cause detriment to genuine whistleblowers will become a thing of the past. This includes ending non-disclosure agreements [NDAs] for whistleblowers.
The Bill is not simply a replacement for the Public Interest Disclosure Act 1998 [PIDA], it will change the landscape and offer an innovative, evidence-based approach based on the four pillars of:
Protection for whistleblowers
Investigations
Accountability
Education ‘
This summary was produced by Steve Turner, RGN, RMN, Ba(Hons), P.G. Dip Ed. Member and former Co-Chair the WhistleblowersUK Healthcare Quality & Safety Focus Group.
About the Author:
Steve began his professional career as a nurse at St George’s Hospital in London in 1981. He also spent a decade working on hospital clinical systems for the American giant Shared Medical Systems, progressing from project manager to Senior Strategic Services Consultant of the U.S. arm of the company. In 1999 he returned to work for the NHS, successfully revamping the Information and Technology department at an NHS Trust prior to a trust merger. A spell in consultancy for a large Cancer Network followed, by leading highly successful multi-organisational projects. In 2002 Steve returned to clinical practice becoming a nurse prescriber in a Mental Health Assertive Outreach Team. In 2014 Steve founded Care Right Now (CIC) a Social Enterprise Company delivering values-based consultancy and developing patient focused clinical education services. The company’s work embraced all of health and social care, ranging from substance misuse to community paediatrics to care homes. Steve is now semi-retired and writing on ‘patient led care’.
About WhistleblowersUK
WhistleblowersUK is the UK’s only Not for Profit organisation. It was set up in December 2014 to provide help, information and support to whistleblowers and in November 2015 launched its campaign for the introduction of an Independent Office of the Whistleblower.
WhistleblowersUK receives no government funding for its work and relies on the generosity of whistleblowers, supporters and the public to maintain its work including support for whistleblowers and development and advancement of policy. Please support us by donating here and by joining our thriving associate membership and getting more involved in transforming whistleblowing.
For more information, please visit the WBUK website: www.wbuk.org or
I am a retired healthcare professional, a nurse prescriber with experience in senior management in both the NHS and private sectors. I worked as a clinician with vulnerable adults on the margins of society.
Over the past two decades I’ve become involved with a situation I was previously unaware of. The widespread marginalisation and victimisation of health and care staff who raise concerns about patient safety and lose their careers as a result. I’ve learned that this problem is part of a much bigger picture which affects all of society, all industries and public sectors, in all countries of the world.
In this blog I reflect on the situation in England based on my experiences and those of the many people I have met as a result. All of whom experienced the backlash that can happen when organisational reputation trumps patient safety. One thing many of us have in common is that, put simply, we never intended to become known as ‘whistleblowers’, we were just trying to do our job to the best of our ability.
In conclusion, I look at key areas to be worked on in order to protect the public and really ‘learn lessons’. These cross all sectors and areas of work. They include the need for changes in legislation, an end to self-regulation in healthcare and elsewhere, and recognition of the value to society of those who risk everything to fight for justice and truth.
A dawning realisation
I began to realise something was seriously wrong when I returned to clinical work in 2002. Having previously worked in senior management (as Head of I.T. in an NHS Trust) and management consultancy, I became concerned that my employer appeared to be putting reputation over patient safety, and if concerns were raised, they were not followed up. I recall looking at Board papers and directions to trusts from the Department of Health [DH] to try and understand this further. One thing I remember is a letter to Chief Executives from the Department of Health which talked about creating an ‘outward facing’ organisation. I didn’t realise at the time what I now see as the real meaning of this, and its link to the ‘no bad news culture’. This involves putting reputation above patient safety.
Later I tried to raise my concerns with a Trust Executive at an early stage, only to be told in both words and body language that the trust didn’t want to hear anything bad. This attitude, and what I saw happening to the team and staff around me, led me to leave the NHS and become self-employed working for the NHS on projects related to medicines and prescribing.
The difficulties continued
Now working as a self-employed contractor I continued to experience difficulties when I spoke up for patients and patient safety. To escalate my concerns I followed the Trust policy, and the appropriate internal routes, including speaking to the Deputy Chief Executive about my concerns. The Deputy CEO was then going to arrange for me to speak to the Non-Executive Director responsible, however the Chair of the Trust blocked me from speaking to them. (This is the Chair who told me they didn’t want to ‘hear anything bad’). Eventually my experiences and increasing frustration led me to make a protected disclosure to the care Quality Commission [CQC] in 2014, in which I set out the patient safety concerns. As a result, the CQC requested that the Trust commission an external investigation of my concerns.
Since being interviewed for the investigation report in 2014 I have heard nothing further. I never saw the investigation report and was never contacted about it. A freedom of information [FOI] request to the CQC produced the response that my concerns were dismissed as ‘all third hand’ (which is incorrect) and I was told that the CQC had ‘lost the report’.
Prior to the FOI request, I was employed as a CQC Specialist Advisor (a zero-hours contract), however following the FOI request this contract was ended without a specific reason being given.
The wider picture in healthcare
I’ve only briefly mentioned some of the aspects of my story here. The most important thing for me was that I found out the common themes behind all genuine healthcare whistleblowers’ stories.
Three things stand out for me.
1. The psychological effect on the whistleblower
I experienced the isolation that whistleblowers are subjected to and the psychological effect this has on individuals. Suddenly you’re on your own, and people you worked with avoid you. In my case, I also kept my distance from some co-workers, as I realised they were being bullied as a result of supporting me.
For me offers of work dried up and a sickening feeling of being ‘sent to Coventry’ set in. In addition to the loss of income, this isolation has a deep effect on my mental health and home life. I believe the approach of employers here is called ‘gaslighting’. It’s deeply troubling.
2. The NHS cold shoulder / being blacklisted
Secondly, I have discovered through meeting other whistleblowers that blacklisting of those who speak out is very common. This can take many forms, ranging from informal blacklisting to interventions to prevent career development, to giving unsolicited (and unfair) bad references.
For those employed by the NHS the Electronic Staff Record [ESR], which is shared throughout the NHS can be used as a way of sharing detrimental information on whistleblowers. This has caused people to be denied a fair chance to gain further employment. I believe the full extent of this is yet to come to light.
In my case the blacklisting took the form of repeatedly being given the ‘cold shoulder’ for example being excluded from meetings; uninvited from regular meetings I was previously part of (without a reason being given); letters and emails not replied to, a higher education establishment being told not to engage with me, and generally being avoided. Of course, this is subjective, and sometimes I may be wrong, as healthcare is a tough work environment. However, I have been subject to some clear examples of ongoing detriment. This lasted right up to, and beyond, my retirement.
On one occasion my company was enthusiastically awarded a contract of work one day, then the very next day the same person ‘phoned me and cancelled the order saying only that it ‘wasn’t what they wanted’. Very strange. Also, I found out years later that staff from the trust I worked for were told not to speak to me, even though in some cases it was to ask me a question about my clinical work.
In addition, I was deeply upset when the NHS Trust, who commissioned one of my projects, failed to acknowledge its success. A poster was presented at the NICE Conference in 2015 and it was highly commended by NICE.
Prior to the Conference, I contacted the trust to let them know of the success and all attempts to engage the trust were ignored. As you can see on the poster (which was produced by NICE) the space for the trust’s logo, on the bottom left, is empty:
In fact, I had several examples of work on the NICE Shared Learning pages, none of which have ever been acknowledged in any way by local NHS Trusts, or any healthcare organisations in Cornwall.
In was fortunate in being successful in delivering the above children’s medicines project, which has had a lasting legacy – the appointment of a Paediatric Community Pharmacist. One of my protected disclosures was about this project. Specifically that I was pressured to alter a report which highlighted the urgent need for improvements in medicines’ safety. At the time there were people in senior positions who backed me up and the report remained unchanged. Since then, all these people have left the trust. More recently the trust was caught up in a ‘governance scandal’ which resulted in the Chief Executive and Board Members who had bullied me leaving suddenly.
3. The effect that the victimisation of healthcare whistleblowers has on patients
Thirdly, as I looked further into the problem, I began to see the full impact that the victimisation of genuine healthcare whistleblowers has on patients. This for me is the most shocking aspect of the problem.
In 2015 I set up the Turn up the Volume! Movement. This was an attempt to bring together all involved in an open and transparent way, with a focus on the core issue of patient safety.
Through this initiative I have met many more people in a similar situation and learned first-hand the effect lack of transparency and denial has on patients. This is well illustrated, for example, in the report of the Gosport Independent Panel Report (2018), where those who raised the alarm were initially listened to, then ignored and their concerns re-labelled as ‘allegations’. As a result of this, in the words of the report, ‘the lives of over 450 patients were shortened while in the hospital’.
Next steps
Based on my experience in trying to link together people in health and care with similar experiences and focus on patients, I believe there are three vitally important areas in healthcare that need addressing.
The need for an individual duty of candour
Firstly, I was shocked to find out that in the NHS the duty of candour (duty to tell the truth), brought in following the Mid Staffordshire inquiry, is an institutional duty of candour. This relies on staff telling the truth to their employer in order to highlight what went wrong. Thanks to the tireless work of campaigner Will Powell the need for an individual legal duty of candour for professionals, managers & leaders in healthcare has been demonstrated. This has parallels to the calls for a ‘Hillsborough Law’. Without this, there is no real mechanism to hold individuals to account for cover-ups and for not being honest.
Making sure initiatives are effective
Secondly, I’m disappointed at the failure to learn and improve patient safety through listening to genuine whistleblowers, whether they be patents or staff, and failure to take measurable actions to change. I believe that the National Freedom to Speak Up [FTSU] Guardian initiative has had unintended negative consequences. Evidence suggests that whilst many trusts are using FTSU to solve problems and make improvements, it is making the situation worse in some trusts, where it is used as a cover for continued victimisation of those who speak out.
Ending self-regulation & providing independent oversight of whistleblowing
Thirdly, in common with industry, I believe that self-regulation in health and care does not work, and the only solution will be to set up a truly independent body to oversee and enforce this. This body must involve patients, who raise concerns at great cost to themselves and their families.
Health regulators in England and the people who they regulate are often uncomfortably close. For example, I was deeply disappointed when I found out only that the CQC Inspector involved in dealing with my concerns raised in 2013, later became employed as Compliance Lead in the same trust.
Background: From 2008 to 2014 my company ran education sessions on managing medicines in a mental health trust. In common with some other mental health trusts the provider also looked after paediatric community services. This is not a mental health service. It covers children with complex health needs including enteral feeding tubes, ventilation, epilepsy and rapidly changing medicines.
Children under the care of this service may be taking in excess of 15 different medicines per day, have complex titration regimes, emergency drugs with associated care plans, plus numerous ‘as required’ (prn) medicines.
It is not unusual for children with complex conditions to be under the care of up to five different providers, and to move between three different providers in one day. For example, from a Home Care Service to the Special School, to a Short Break House, also being seen in an Outpatient Clinic on the same day too. As a result, parents frequently have to repeat the information on their child’s medicines every time they move to another service, or a new person is involved.
Where to start? The idea for change came about because of concerns that the staff in Children’s Short Break Houses were not learning what they needed about children’s medicines, as the learning was geared to the majority of staff who worked in mental health. So a new learning package for children’s staff was commissioned.
Part of the work to design the learning package included a baseline assessment which was conducted with parents and staff. This soon revealed that training alone was not the answer. It showed delays in medicines information reaching GPs, workarounds for obtaining information in order to administer medicines in the houses and a general lack of confidence in the whole process.
As a result, we looked at the whole system starting with the area where most concerns had been raised, which was having an up-to-date complete list of a child’s medicines available at all times (medicines reconciliation). The system in place for Short Break Houses involved paying a local GP (not usually from the child’s GP Practice) to write up a medicines chart for each child. The process was fraught with difficulties and delays and widely disliked by everyone directly involved.
So we set about looking for a new way to manage the lists of medicines with more training and more input for the staff in the services involved. We came up with a new (and much more robust) process for medicines reconciliation in the Short Break Houses. This was fully documented in a new policy and involved cross-checking by both the staff and the parents.
Just before this went live, we asked the parents to review and comment on it and they said: ‘If you’re producing an accurate and up-to-date list of my child’s medicines, why keep it the Short Break House, can’t it go with my child?’ So, the My Medicines chart, which travels with the child, was born.
What was involved? The My Medicines process led to the design and production of a new chart which has to be signed and checked by the parents. It resulted in 40 children with complex conditions being offered a hand held paper record of their medicines (produced and validated by clinicians), which they take around with them wherever they go.
Benefits: The new process, which continues to evolve, means that the child’s GP is now directly involved in day-to-day medicines reconciliation (they weren’t before); the parents are always asked to check and sign the charts (they weren’t before); verbal messages about medicines are never taken, and incomplete (or missing) directions are rapidly rectified (never worked around).
Some specific benefits of the new process included: • It reduced the risks of error, by providing full and accurate information on children’s medicine across their entire pathway. • It cut out the need for parents to keep having to repeat what medicines their child is taking to different professionals and care agencies. • It freed up medical and clinical time which was previously spent chasing missing information. • It reduced the number of third-party handovers and transcribing of prescription information.
Looking back, it’s hard to believe that the old ways of working, which caused so many difficulties (especially for front line staff), were carried out for so long. These risky practices, or similar, are believed to still be commonplace in England.
Revealing hidden incidents and near misses:
In the first month of the project we raised 17 medicines incidents or near misses. Of these 11 related to problems with communication of information across the child’s pathway.
Resolving these has resulted in improved communication and engagement between different clinical groups and providers, and a desire from all quarters to take the project further. Previously many of these incidents were not logged or tracked across organisations. In some cases, it was only due to the vigilance of the staff and parents that they were spotted, and errors avoided.
Accepting the changes:
The project was well received by parents and staff and resulted in improved communication and engagement between different clinical groups and providers. This included the Consultant Paediatricians (working for the secondary care provider), who were initially sceptical.
The project was less well received by the relevant medicines and prescribing committees, who were understandably concerned about who owned the My Medicines chart and had agreed to its content. Explaining this was made more difficult because it is hard to get across the complexity of the arrangements, due to the critical nature of the children’s illnesses, in a committee setting.
I make no apologies for ensuring from the outset that it was the parents who owned the charts, which were designed by the project team (not a committee) to meet all best practice standards. It always worries me that when it comes to cross- organisational working the formal committees and systems in place can inadvertently act as a barrier to safety rather than promoting it. There is no doubt we had designed a safer process and my company was happy to take accountability for any associated risks.
As a legacy of the project, a Community Paediatric Pharmacist was appointed specifically to work with this group of children. So whatever evolves will now be based on inter-disciplinary thinking and working and will have clear safety parameters. I am grateful for the enlightened thinking of the leaders who commissioned this work and supported this novel approach.
Steve Turner RGN, RMN, Ba (Hons), P.G. Dip. Ed.
This example was included as a NICE Shared Learning resource and was highly commended by NICE in 2015.
Prescribing psychotropic medicines for people with learning disabilities / autism who show symptoms of distress*
( #jargonbuster – psychotropic medicines = The phrase “psychotropic drugs” is a technical term for psychiatric medicines that alter chemical levels in the brain which impact mood and behaviour. Often referred to as anti-psychotic medicines).
Summary:
People with learning disabilities and / or autism can be prescribed antipsychotic medicines for reasons other than to treat psychosis. This is a complex area that involves detailed knowledge off the patient and inclusion of everybody concerned with their care. This includes parents relatives and carers and must involve anyone with power of attorney [LPA] or a Court of Protection Deputyship. This piece sets are some of the key areas to consider when prescribing in the form of an aide memoire. It is important to note that the art and science of prescribing is not simply about writing a prescription. It is also prescribing decision if a medicine is stopped, changed or the dose altered, or if a non-medical option is chosen. Avoiding unnecessary prescribing should be an absolute priority and all guidelines refer to this. On the other hand, some patients require unusual medicines regimes. If this is the case, then the reasons for this must be fully documented as part of a multidisciplinary process including best interest decision-making. This must then be regularly monitored and reviewed.
Key points:
Facts:
Most of the prescribing in this area is ‘off label’( #jargonbuster – that’s medicines prescribed for something that isn’t listed as an ‘indication’ for that medicine, or is over/under the recommended dose).
This prescribing can include multiple anti-psychotic medicines, often medicines in the same class.There is a limited evidence base for this type of prescribing. Concurrent prescribing of this nature renders the medicines off-label.
Psychotropic medicines in people with learning disabilities / autism who show symptoms of distress* should be initiated by an appropriate specialist, after which they are not always prescribed by a specialist in this area.
Diagnostic overshadowing may lead to inappropriate prescribing.
Diagnostic overshadowing is the attribution of a person’s symptoms to their mental condition, when such symptoms actually suggest a comorbid condition.
Actions to take for each person:
A Holistic assessment including taking all measures possible to understand why the person may be distressed, and taking actions to alleviate this, based around the person.*
Ensure that the prescribing takes into account the tests and monitoring required for safe prescribing, and takes into account the latest national and local guidelines.
Before prescribing it’s important to understand all triggers and environmental factors. Plus the reasons for behaviour now and what has happened in the past, including what works well and what acts as triggers*.
There are ongoing concerns that psychotropic drugs are used inappropriately in people with intellectual disability. [2]
After exploring ALL options, if medicine is thought to be the answer:
Ask about allergies, sensitivities and adverse reactions to medication. Check the documentation on this and ensure it’s recorded accurately (e.g. if the person has reacted to a drug is the nature of the reaction recorded in full, and has it been shared with all involved in the person’s care).
Take into account views of family and carers.
Take into account any advance decisions and support plans.
Take care to avoid diagnostic overshadowing.
Ensure there is specialist initiation and review of the prescribing.
Ensure Multi-Disciplinary team involvement & inter-organisational involvement.
If the prescribing deviates from guidelines (for example around tests and monitoring required and dosage) this must be documented, with a reason.
Act in accordance with the Mental Capacity Act [MCA] , where capacity to make a specific decision is lacking. (NB: Mental Capacity assessments must be time and decision specific).
Best interests decisions must involve all parties, be fully documented & regularly reviewed. This includes involving people who have Lasting Power of Attorney [LPA] or are Court of Protection Deputies.
Where appropriate, use a tiered approach to prescribing – ‘start low, go slow’.
Ensure involvement of Second Opinion Appointed Doctors (SOADs#) to provide a statutory safeguard where consent is an issue.
Follow up and monitoring:
Confirm the monitoring required and ensure a process is in place for this.
#‘SOADs visit the person and explore the current and proposed treatment, certifying what is considered to be appropriate and reasonable in circumstances where the person cannot or does not consent to it, discussing it with team members and the person before reaching their conclusions.’
Clear documentation is vital:
Of the holistic assessment
Of the condition that’s being treated by the medicine(s)
Of the indication for each medicine (i.e. what it is being prescribed for) is explicitly documented, and this information is available to everyone involved in their care.
Of possible precipitating factors and measures that help the person*
Of patient involvement
Of carer and family involvement
Of multi-disciplinary team involvement
Of the decision making process and rationale for any best interests decision(s).
Of the rationale for prescribing / not prescribing
Including review dates and evidence of reviews
Real time monitoring of the effect of the medicine(s), including any as required ‘prn’ medicines.
Documenting evidence of changes in response to the medicine(s) not being as expected, including if the medicines has no effect, and the actions taken on this.
Personal views of Steve Turner RGN; RMN; Ba (Hons); P.G. Dip Ed Feedback and views welcome, send them to carerightnow@gmail.com
Steve is a retired nurse prescriber, former Head of Medicines and Prescribing for @MedicineGov , former Associate Lecturer at Plymouth University and a former NICE Medicines and Prescribing Programme Associate.
Version 7 Dated 25.11.2024
Revision history:
25/11/2024
Out of date links removed, information sources updated, some text & links removed. Extra explanatory text added.
03/05/18
*Following feedback from parents & carers I’ve changed some wording and added some additional wording which puts the patient first. Thank you for the feedback.
12/12/2018
Updated with link to the RPS Competency Framework for all Prescribers, following feedback from readers.
09/01/2019
Updated to include reference to diagnostic overshadowing.
14/01/2019
Updated to include allergies, sensitivities adverse reactions and feedback from teaching sessions.
15/01/2018
Updated to include specific mention the Mental Capacity Act.
20/04/2019
Notes that medicines related option should only be considered if non-medical options have not worked. Minor amendments to text.









{kind=link}