In producing a teaching session on evidence based medicine, it occurred to me that there are some important points everyone needs to know, and that they are summarised well in these videos from James McCormack. So, if you like learning through the medium of song and dance, these are for you 😃.
There are some links to important guidelines and academic references too. Some of the comments on learning points reflect my personal views.
Assessing the evidence
‘Viva La Evidence’ from James McCormack
Key learning points:
Look for absolute numbers.To assess clinical studies, you need to have sight of the ‘absolute numbers’ and the figure for Absolute Risk Reduction [ARR]. Sales and marketing people may just tell us about Relative Risk Reduction [RRR]. This figure stays constant with different populations, and always looks better. To be honest I find this concept easy to understand but hard to explain. Here’s a link to an article which goes into more detail.
POOs and DOOs. It’s helpful to look closely at the relevance of the research for patients. Is it focused on outcomes that are patient-oriented [POOs] or disease-oriented outcomes [DOOs]? Click here for a related article.
‘The End of Guidelines’ – how useful are they in real life
‘The end of Guidelines’ – from James McCormack
Key learning point:
Guidelines not tramlines
Most current guidelines are written for specific diseases and conditions when, in reality, many people often have more than one long-term condition. In fact, most people with chronic conditions, and most people over 65, have multiple health conditions. This together with other factors such as past experiences, health beliefs, ethnicity, poverty, lifestyle and cultural factors, will influence the choice of medicines.
To help with this there are some important NICE Guidelines, which should be cross-referenced in practice guidance (local and national).
All prescribers should be familiar with and use these guidelines in helping patients choose medicines & treatments. This includes the patient’s choice not to take a medicine, which is specifically noted in the NICE Guideline on Medicines Adherence.
Guidelines are just that – ‘guidelines’ – and not to be followed blindly without question or reference to the individual patient.
The clinician’s role has changed from being the ‘expert’ to that of a teacher, advisor, mentor and sometimes an advocate. At the end of the day, in everyday situations, what we do is our decision. The much-used phrase ‘shared decision making’ is inappropriate in my view, it stems from the old fashioned ‘doctor knows best’ attitude. I prefer to use the phrase patient led decision making.
Following on from my blog on making the most of remote consultations, I realised it would be helpful to talk about the outcome patients should expect from consultations (wherever they are conducted). This blog is based on my clinical experience, on feedback from patients, carers and relatives, and on my experience of helping look after my mother at the end of her life.
There are some simple things that everyone should come away with at the end of a consultation. Knowing the plan & what the next steps are. Where to find information on what has been discussed and what to do if things get worse. If this information isn’t made clear, ask ‘what’s the plan?’
Consultation information:
At the end of the consultation, you must:
Have agreed a plan (even if this is ‘watch and wait’, or a referral on)
Have written information on what has been discussed& where to find support
Know the signs of improvement or the signs of deterioration to look for
Know when & who to contact if things change
Know who to contact in an emergency
At the end of the consultation:
At the end of the consultation, you should know:
That your concerns have been listened to
That the agreed actions will be taken
That you can seek a second opinion if needed
That the consultation will be communicated to all involved in the patient’s care
You should also receive:
Written information on the consultation. This may be in the form of notes, a care plan or visit summary & copies of ALL communication between clinicians.
‘If you’re not provided your records (as you should be), you may wish to keep a record of your consultations yourself and / or record them. As a clinician I encourage this.’ – Steve Turner RGN; RMN; Ba(Hons); P.G. Dip. Ed
In a future blog I’ll look at communication and documentation. What form should this take? Covering all options including online access to records, patient-held notes, visit summaries, assessment letters, patient notebooks, body maps, recordings, images. How can we ensure patients & all involved have this information in real time?
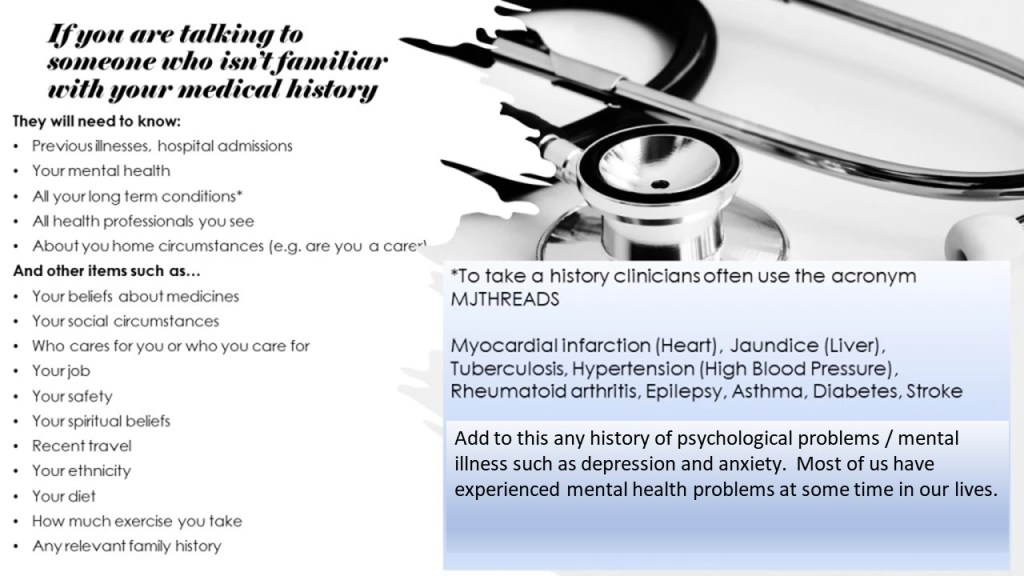
It is often assumed that the person carrying out a consultation has access to your medical records and your full medical history. Sometimes consultations are carried out with a clinician who doesn’t know (or have access to) your medical history.
Multimorbidity – what this means and why it matters
Many of us have more than one long-term medical problem (‘multimorbidity’ in jargon). As we get older this becomes inevitable. Services are frequently delivered by different specialists from a variety of different professions, so it’s important to share everything in order to ensure the treatments recommended are compatible.
Important things we can forget to mention
If we have a medical condition that has been ongoing for many years and is well controlled, we may forget to tell the clinician. You may forget to mention something like asthma for example, because it hasn’t been problematic for a while. It’s really important not to miss these areas, as the safety and effectiveness of your treatment plan depends on it.
Being prepared for a consultation - a checklist
It may help, before the consultation, to write a list of:
Allergies, sensitivities and adverse reactions to medicines & treatments.
All your long term conditions (the chart below shows an acronym ‘MJTHREADS’ used by clinicians). Alternatively it may be helpful to think of a ‘systems review’ in terms of a ‘body scan’, starting with the head.
All health related people (including complementary therapists, & support groups) that you see.
In addition some (or all) of the following details will be relevant. Think about:
Your preferences and beliefs about treatments, including resuscitation & end of life care (often called advanced decisions or advance care plans).
Who cares for you or who you care for. People don’t always realise (or tell clinicians) that they are caring for others.
Your job , or how you occupy your time.
Financial worries.
Your social circumstances – who do you live with? -do you have close family & friends? -do you feel isolated? -live in a remote location? – do you feel vulnerable? – your hobbies?
How you feel about your own safety – have you ever felt like harming yourself?
Past (or recent / ongoing) trauma and abuse.
Your spiritual beliefs.
Recent travel abroad.
Your ethnicity.
Your diet and any recent changes.
Recent weight loss or weight gain.
How much exercise you take.
Your sleep pattern and any recent changes.
Your family history.
Other areas (listed here in no specific order) such as childhood history, pregnancy history, risk taking history or sexual history.
The above list may look daunting, and is obviously not all needed in all consultations, however it’s worth reviewing. I have come across people who were waiting to be asked some of the above questions, and wanted to tell someone something important, who told me they only opened up because they were asked.
*In response to feedback on this blog from patients, it’s important to note that there may be some details related to mental health that patients do not want to share with all clinicians.
Medicines errors in care homes are unacceptably high. A key study found that residents taking seven or more medicines had a 79% chance of being victim of a medicines error (Alldred et all 2009).This led to several follow-up studies and actions to improve medicines management in care homes, including a move to implement electronic medicines administration [eMAR] systems. A recent study explored medication-related incidents and their causes in UK care homes. This review emphasised the need for improved medication management processes to reduce errors and enhance patient safety (Irons et al 2022).
Best practice in medicines record keeping
The management of medicines in nursing and residential homes is part of a highly complex pathway. It involves multiple staff groups and organisations.
These include the G.P.; all who prescribe medicines and treatments; Care Staff of all grades; Support Workers; Consultants; Specialist Practitioners; and Pharmacists.
Benefits of electronic MAR charts
The benefits of implementing electronic MAR charts fall into three categories.
Improved legibility.
Improved access (e.g., if the charts are accessed and updated on a computer or portable device there is less risk of losing, damaging, or mislaying them).
eMAR chart systems that obtain the data taken directly from the Community Pharmacy system eliminate the need for transcribing.
Systematic reviews indicate that carefully planned and implemented eMAR systems contribute to a decrease in medicines errors, reduced administrative costs and improved quality of care (Gates et al 2021).
Challenges of implementing electronic MAR charts
There are three ‘bottom line’ challenges to manage when transitioning to electronic MAR charts.
1. Assessing potential eMAR systems. Thisis critical, as poorly designed systems will not deliver benefits, and eventually fail. The system must be easy to use and free of unnecessary jargon, using only approved acronyms or mnemonics. Electronic systems also offer the opportunity to introduce features which enhance safety, some of which, such as time ordered charts, are difficult to include in a paper-based syste
Here’s a some key features to look for:
Photo identification
Time ordered charts
Body maps
Drug images
Start and finish dates
Insulin charts
Warfarin charts
As required – prn- charts
Does the system record the reason prn medicines were given?
Medication history
Medication profiles
How the system records allergies and sensitivities
What alerts and warning messages are included?
How the system copes with medicines dispensed directly from hospitals
How does the system cater with titration of medicines and variable doses
How does the system cater with weekly medicines (e.g. alendronic acid)?
Use of monitoring information (e.g. INR for warfarin administration, lithium level recording, BMI, B/P, pulse etc.)
That the system uses up to date approved terminology
Does the system records medicines not given or partially administered, with a reason?
How the system can be used to order and control stocks of medicines
How easy is it to produce reports from the system?
2. Data Security and Protection. It is vital that the system handles patient consent; patient confidentiality, system access; ownership of patient identifiable data; storage and transfer of data in a way which is compliant with the laws and regulations of your part of the U.K.
All organisations and systems that access to NHS patient data must successfully complete the NHS data security and protection toolkit [DSPT]. This toolkit provides assurance that the system suppliers are handling data safely and that personal information is handled correctly. You can search the supplier’s NHS DSPT registration here: https://www.dsptoolkit.nhs.uk/OrganisationSearch
3. Process Reviews. It is important to look at your current processes and how the new system will work. For example, there have been problems where urgent acute prescriptions were supplied by a different pharmacy from the pharmacy linked to the home’s eMAR system. The eMAR system must be able to cope with all aspects of prescribing from multiple sources and prevent information having to be duplicated.
Training and support requirements
Quality training and support, both during the implementation and on an ongoing basis, underpin all successful healthcare I.T systems. There are four areas which are sometimes overlooked that deserve special mention:
1. Many of the users of eMAR systems will be Healthcare Assistants or other non-registered skilled staff. As a result, it will be important that the training they receive reinforces their duty to keep accurate records, that they know where to go for help and advice and their role and responsibilities are made clear.
2. A substantial number of staff may speak English as a second language. Therefore, it is important that eMAR systems do not use any unnecessary jargon, and that any help text is in plain language.
3. Appropriate knowledge of Data Protection (GDPR) and Information Governance rules and regulations is essential and should be built into any training programmes.
Overall, consideration needs to be given to the nature and content of the training needed to implement the system, including how this is linked to the policies and procedures and overall governance of the home.
Good suppliers will be able to give advice and support on this.
Conclusion
Record keeping in medicines management is a critical safety area for care homes. The current high level of medicines errors is in care homes affects half a million people in England.
The prospect of implementing electronic systems for recording medicines administration holds great potential but is not itself without risk. It needs to be approached carefully in the light of the complex arrangements and multiple organisations involved in prescribing, supplying, administering, dispensing and monitoring medicines for your residents.
Given the considerations over choice and implementation of systems, eMAR can overcome problems of legibility, transcribing, and access to records and information in a way which is not possible with paper systems.
In years to come it is likely that, just as most G.P.’s would not want to return to paper systems, care homes will come to see electronic systems in the same way. The main beneficiary of this will be the residents in terms of improved safety.
References:
Alldred P, Barber N, Buckle P et al (2009) Care home use of medicines study (CHUMS): Medication errors in nursing and residential care homes – prevalence, consequences, causes and solutions. Report to the Patient Safety Research Portfolio. Department of Health, London.
Peter J Gates, Rae-Anne Hardie, Magdalena Z Raban, Ling Li, Johanna I Westbrook, How effective are electronic medication systems in reducing medication error rates and associated harm among hospital inpatients? A systematic review and meta-analysis, Journal of the American Medical Informatics Association, Volume 28, Issue 1, January 2021, Pages 167–176, https://doi.org/10.1093/jamia/ocaa230
Irons, M. W., Auta, A., Portlock, J. C., & Manfrin, A. (2022). Medication errors and processes to reduce them in care homes in the United Kingdom: a scoping review. Home Health Care Services Quarterly, 41(2), 91–123. https://doi.org/10.1080/01621424.2021.2007196
Author: Steve Turner RGN, RMN, Ba (Hons), PG Dip Ed – a retired experienced nurse educator, who has worked in strategic consultancy and on change projects across healthcare in the UK.