Following on from my blog on making the most of remote consultations, I realised it would be helpful to talk about the outcome patients should expect from consultations (wherever they are conducted). This blog is based on my clinical experience, on feedback from patients, carers and relatives, and on my experience of helping look after my mother at the end of her life.
There are some simple things that everyone should come away with at the end of a consultation. Knowing the plan & what the next steps are. Where to find information on what has been discussed and what to do if things get worse. If this information isn’t made clear, ask ‘what’s the plan?’
Consultation information:
At the end of the consultation, you must:
Have agreed a plan (even if this is ‘watch and wait’, or a referral on)
Have written information on what has been discussed& where to find support
Know the signs of improvement or the signs of deterioration to look for
Know when & who to contact if things change
Know who to contact in an emergency
At the end of the consultation:
At the end of the consultation, you should know:
That your concerns have been listened to
That the agreed actions will be taken
That you can seek a second opinion if needed
That the consultation will be communicated to all involved in the patient’s care
You should also receive:
Written information on the consultation. This may be in the form of notes, a care plan or visit summary & copies of ALL communication between clinicians.
‘If you’re not provided your records (as you should be), you may wish to keep a record of your consultations yourself and / or record them. As a clinician I encourage this.’ – Steve Turner RGN; RMN; Ba(Hons); P.G. Dip. Ed
In a future blog I’ll look at communication and documentation. What form should this take? Covering all options including online access to records, patient-held notes, visit summaries, assessment letters, patient notebooks, body maps, recordings, images. How can we ensure patients & all involved have this information in real time?
It is often assumed that the person carrying out a consultation has access to your medical records and your full medical history. Sometimes consultations are carried out with a clinician who doesn’t know (or have access to) your medical history.
Multimorbidity – what this means and why it matters
Many of us have more than one long-term medical problem (‘multimorbidity’ in jargon). As we get older this becomes inevitable. Services are frequently delivered by different specialists from a variety of different professions, so it’s important to share everything in order to ensure the treatments recommended are compatible.
Important things we can forget to mention
If we have a medical condition that has been ongoing for many years and is well controlled, we may forget to tell the clinician. You may forget to mention something like asthma for example, because it hasn’t been problematic for a while. It’s really important not to miss these areas, as the safety and effectiveness of your treatment plan depends on it.
Being prepared for a consultation - a checklist
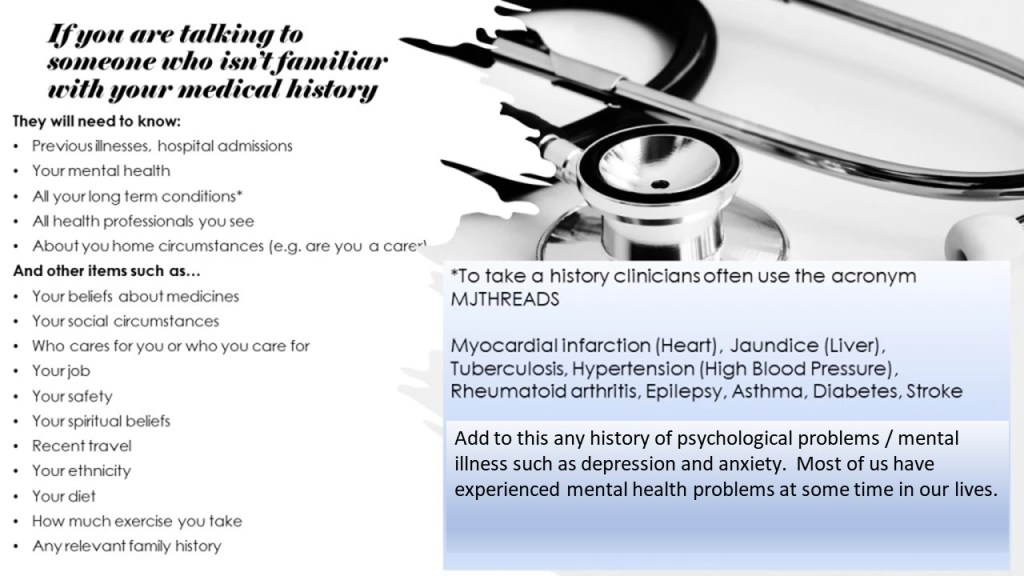
It may help, before the consultation, to write a list of:
Allergies, sensitivities and adverse reactions to medicines & treatments.
All your long term conditions (the chart below shows an acronym ‘MJTHREADS’ used by clinicians). Alternatively it may be helpful to think of a ‘systems review’ in terms of a ‘body scan’, starting with the head.
All health related people (including complementary therapists, & support groups) that you see.
In addition some (or all) of the following details will be relevant. Think about:
Your preferences and beliefs about treatments, including resuscitation & end of life care (often called advanced decisions or advance care plans).
Who cares for you or who you care for. People don’t always realise (or tell clinicians) that they are caring for others.
Your job , or how you occupy your time.
Financial worries.
Your social circumstances – who do you live with? -do you have close family & friends? -do you feel isolated? -live in a remote location? – do you feel vulnerable? – your hobbies?
How you feel about your own safety – have you ever felt like harming yourself?
Past (or recent / ongoing) trauma and abuse.
Your spiritual beliefs.
Recent travel abroad.
Your ethnicity.
Your diet and any recent changes.
Recent weight loss or weight gain.
How much exercise you take.
Your sleep pattern and any recent changes.
Your family history.
Other areas (listed here in no specific order) such as childhood history, pregnancy history, risk taking history or sexual history.
The above list may look daunting, and is obviously not all needed in all consultations, however it’s worth reviewing. I have come across people who were waiting to be asked some of the above questions, and wanted to tell someone something important, who told me they only opened up because they were asked.
*In response to feedback on this blog from patients, it’s important to note that there may be some details related to mental health that patients do not want to share with all clinicians.
Prescribing psychotropic medicines for people with learning disabilities / autism who show symptoms of distress*
( #jargonbuster – psychotropic medicines = The phrase “psychotropic drugs” is a technical term for psychiatric medicines that alter chemical levels in the brain which impact mood and behaviour. Often referred to as anti-psychotic medicines).
Summary:
People with learning disabilities and / or autism can be prescribed antipsychotic medicines for reasons other than to treat psychosis. This is a complex area that involves detailed knowledge off the patient and inclusion of everybody concerned with their care. This includes parents relatives and carers and must involve anyone with power of attorney [LPA] or a Court of Protection Deputyship. This piece sets are some of the key areas to consider when prescribing in the form of an aide memoire. It is important to note that the art and science of prescribing is not simply about writing a prescription. It is also prescribing decision if a medicine is stopped, changed or the dose altered, or if a non-medical option is chosen. Avoiding unnecessary prescribing should be an absolute priority and all guidelines refer to this. On the other hand, some patients require unusual medicines regimes. If this is the case, then the reasons for this must be fully documented as part of a multidisciplinary process including best interest decision-making. This must then be regularly monitored and reviewed.
Key points:
Facts:
Most of the prescribing in this area is ‘off label’( #jargonbuster – that’s medicines prescribed for something that isn’t listed as an ‘indication’ for that medicine, or is over/under the recommended dose).
This prescribing can include multiple anti-psychotic medicines, often medicines in the same class.There is a limited evidence base for this type of prescribing. Concurrent prescribing of this nature renders the medicines off-label.
Psychotropic medicines in people with learning disabilities / autism who show symptoms of distress* should be initiated by an appropriate specialist, after which they are not always prescribed by a specialist in this area.
Diagnostic overshadowing may lead to inappropriate prescribing.
Diagnostic overshadowing is the attribution of a person’s symptoms to their mental condition, when such symptoms actually suggest a comorbid condition.
Actions to take for each person:
A Holistic assessment including taking all measures possible to understand why the person may be distressed, and taking actions to alleviate this, based around the person.*
Ensure that the prescribing takes into account the tests and monitoring required for safe prescribing, and takes into account the latest national and local guidelines.
Before prescribing it’s important to understand all triggers and environmental factors. Plus the reasons for behaviour now and what has happened in the past, including what works well and what acts as triggers*.
There are ongoing concerns that psychotropic drugs are used inappropriately in people with intellectual disability. [2]
After exploring ALL options, if medicine is thought to be the answer:
Ask about allergies, sensitivities and adverse reactions to medication. Check the documentation on this and ensure it’s recorded accurately (e.g. if the person has reacted to a drug is the nature of the reaction recorded in full, and has it been shared with all involved in the person’s care).
Take into account views of family and carers.
Take into account any advance decisions and support plans.
Take care to avoid diagnostic overshadowing.
Ensure there is specialist initiation and review of the prescribing.
Ensure Multi-Disciplinary team involvement & inter-organisational involvement.
If the prescribing deviates from guidelines (for example around tests and monitoring required and dosage) this must be documented, with a reason.
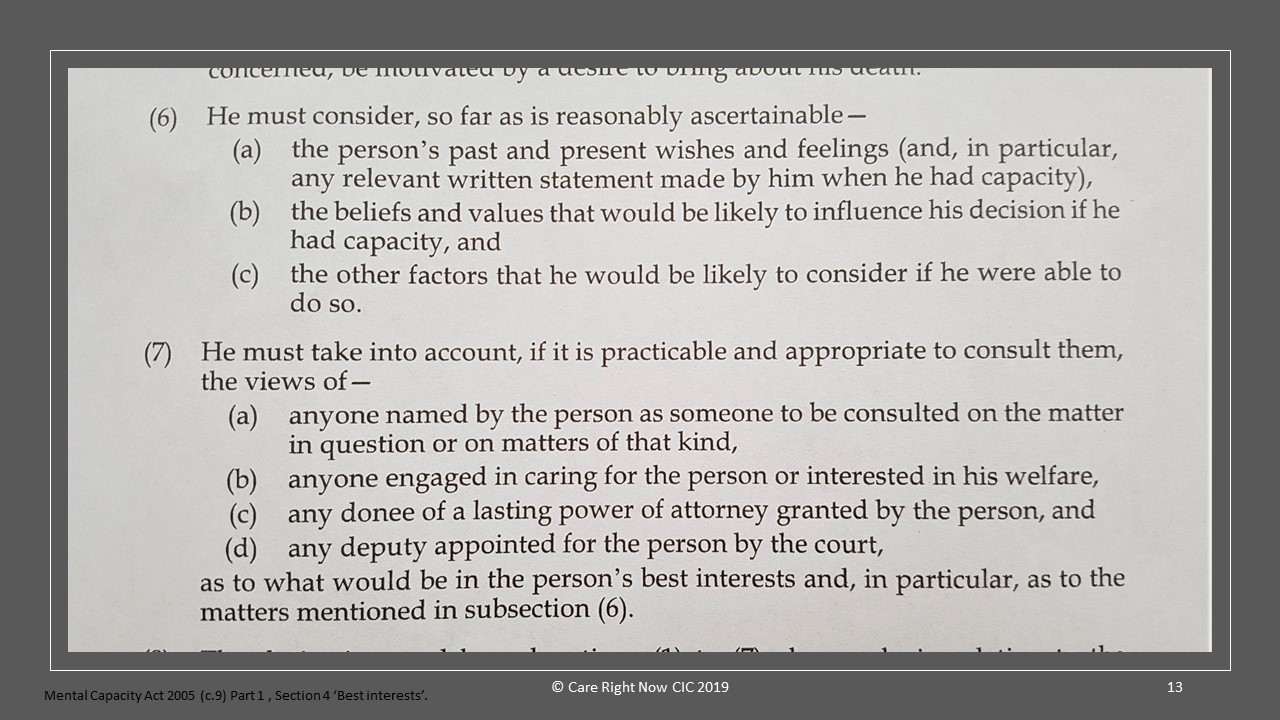
Act in accordance with the Mental Capacity Act [MCA] , where capacity to make a specific decision is lacking. (NB: Mental Capacity assessments must be time and decision specific).
Best interests decisions must involve all parties, be fully documented & regularly reviewed. This includes involving people who have Lasting Power of Attorney [LPA] or are Court of Protection Deputies.
Where appropriate, use a tiered approach to prescribing – ‘start low, go slow’.
Ensure involvement of Second Opinion Appointed Doctors (SOADs#) to provide a statutory safeguard where consent is an issue.
Follow up and monitoring:
Confirm the monitoring required and ensure a process is in place for this.
#‘SOADs visit the person and explore the current and proposed treatment, certifying what is considered to be appropriate and reasonable in circumstances where the person cannot or does not consent to it, discussing it with team members and the person before reaching their conclusions.’
Clear documentation is vital:
Of the holistic assessment
Of the condition that’s being treated by the medicine(s)
Of the indication for each medicine (i.e. what it is being prescribed for) is explicitly documented, and this information is available to everyone involved in their care.
Of possible precipitating factors and measures that help the person*
Of patient involvement
Of carer and family involvement
Of multi-disciplinary team involvement
Of the decision making process and rationale for any best interests decision(s).
Of the rationale for prescribing / not prescribing
Including review dates and evidence of reviews
Real time monitoring of the effect of the medicine(s), including any as required ‘prn’ medicines.
Documenting evidence of changes in response to the medicine(s) not being as expected, including if the medicines has no effect, and the actions taken on this.
Personal views of Steve Turner RGN; RMN; Ba (Hons); P.G. Dip Ed Feedback and views welcome, send them to carerightnow@gmail.com
Steve is a retired nurse prescriber, former Head of Medicines and Prescribing for @MedicineGov , former Associate Lecturer at Plymouth University and a former NICE Medicines and Prescribing Programme Associate.
Version 7 Dated 25.11.2024
Revision history:
25/11/2024
Out of date links removed, information sources updated, some text & links removed. Extra explanatory text added.
03/05/18
*Following feedback from parents & carers I’ve changed some wording and added some additional wording which puts the patient first. Thank you for the feedback.
12/12/2018
Updated with link to the RPS Competency Framework for all Prescribers, following feedback from readers.
09/01/2019
Updated to include reference to diagnostic overshadowing.
14/01/2019
Updated to include allergies, sensitivities adverse reactions and feedback from teaching sessions.
15/01/2018
Updated to include specific mention the Mental Capacity Act.
20/04/2019
Notes that medicines related option should only be considered if non-medical options have not worked. Minor amendments to text.



 youtube.com/@SteveTurnerCareRightNow
youtube.com/@SteveTurnerCareRightNow