
Managing medicines in care homes – implementing Quality Standards.
This blog is designed to provide information for care homes and for those choosing a care home.
In a previous blog I looked at the implications of implementing the NICE Guideline on Managing Medicines in Care Homes.
As with all my posts this is a ‘rolling blog’. I welcome feedback and comments. I will take into account all feedback and use the blog to share new learning. If I’ve missed anything or I am wrong on something I will share the learning.
Some tips:
1. Care Homes must have a medicines policy that is regularly reviewed.
It’s worth considering how your policy links to staff training and how user friendly it is. Are procedures outlined clearly in the policy, do they link to competency assessments, and do you use checklists?
For example, we recently helped a care home produce a checklist of the key information needed when contacting a doctor. It is based on the SBAR (situation-background- assessment-recommendation) principle to help focus on the key information. This is proving popular as it saves time on the ‘phone, and the structured approach is popular with GPs. Staff commented that it has saved them hours of chasing, has improved responsiveness & their relationship with local services.
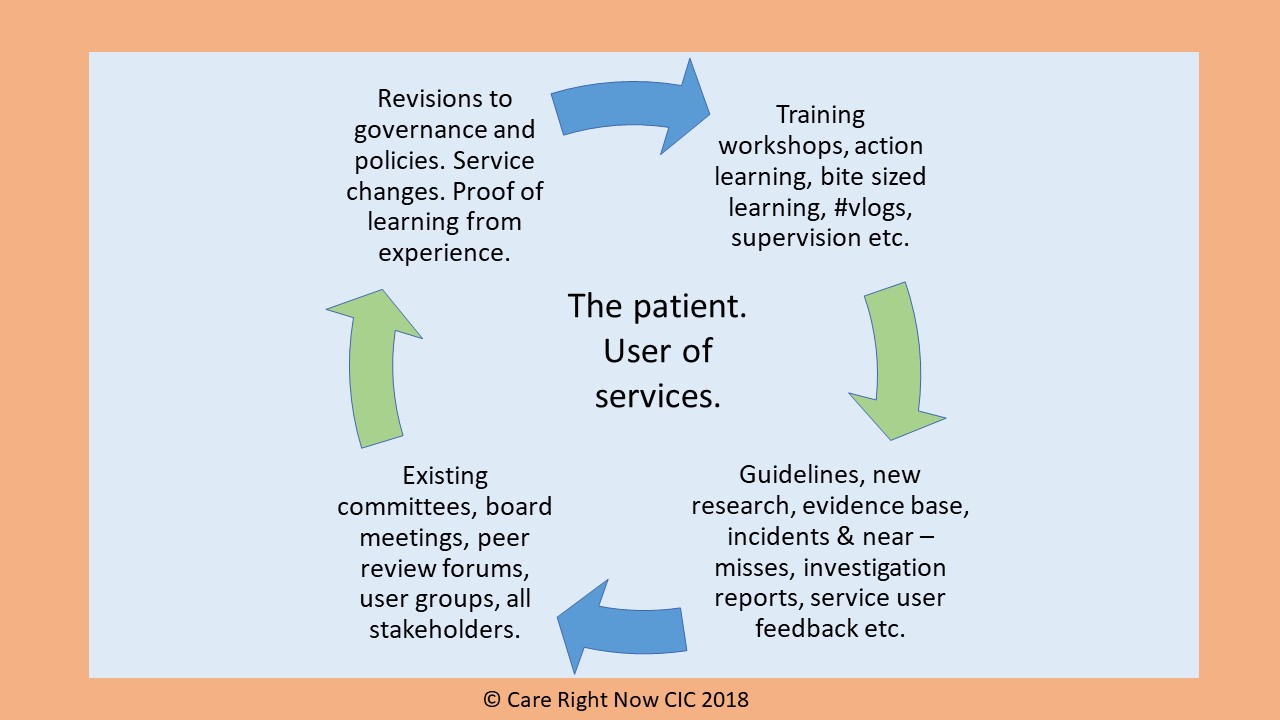
Here’s our method of working. It’s not rocket science and it works. I recommend this approach.
2. People must have an accurate listing of their medicines on the day they transfer to the care home.
This is an area where care home staff are dependent on others. Hours can be spent trying to sort out problems. My advice here is for managers to ensure that discrepancies are always reported back to the source (in writing) and ask for feedback on how they are followed up. Additionally, it’s helpful to record your satisfaction with good quality and complete discharge information.
Our experience is that electronic systems can greatly improve quality of this information.
An NHS Patient Safety Alert highlights the importance of communication of discharge information.
3. People who live in care homes should have at least 1 multidisciplinary medication review per year.
There is considerable variation in practice around medicines reviews, with increasing help available from Clinical Commissioning Group Medicines Management Teams and Specialist Clinicians in most areas.
Although this is an area largely outside the control of care homes there are 3 things which can help.
- Firstly, by consistently referring back any prescriptions which don’t have complete and unambiguous directions.
- Secondly, by ensuring that there is an easily accessible record of what each medicine is being prescribed for, (regular medicines, one-off prescriptions and as required medicines). I am still amazed that this isn’t always the case.
- And thirdly, whilst staff residents / relatives are not expected to be experts on medicines, access to basic information on each medicine, including on side-effects and interactions should be readily available.
4. Ensure you have safe systems for administering and recording medicines.
It is vital that you have a reliable and auditable system of MAR [medicine administration record] charts in place and that the process of administration of medicines to residents is safe.
Two main points spring to mind:
4.1. Monitored dose systmes [MDS] vs original pack dispensing [OPD].
There has been a move by some Pharmacies & local NHS teams to change residential homes from Monitored Dose Systems [MDS] (also called blister packs) back to Original Pack Dispensing [OPD] (sometimes referred to as ‘patient pack dispensing’). The reason for this is often given as to improve safety. It is sometimes implied that guidelines are driving this move back to original pack dispensing, even that OPD can help prevent polypharmacy & reduce medicines waste. All these statements are misleading.
Interestingly, the cost to the Pharmacy of putting the medicines in MDS blister packs is not mentioned in their promotions original pack dispensing [OPD].
I have not been able to find any clear evidence that original pack dispensing is safer than monitored dose systems. Additionally, the related NICE guidelines, quality standards and the CQC report ‘Medicines in Health and Social Care’ do not state this.
What’s important is that the home uses the safest system of delivering medicines to the residents, considering the patients’ wishes, the home’s skill mix, staff competencies, workload, and capacity. This is particularly important as staff tell me the original pack dispensing takes ‘twice as long’.
My advice on the subject of MDS vs OPD is that if you are being lobbied to change to original pack dispensing, here are some key questions to consider:
A. Bearing in mind that OPD could take twice as long, what are the advantages of moving to this? Can you be sure, for example, that unsafe practices such as ‘potting up’ will not creep into use? Will it improve patient safety & compliance with NICE Guidelines and quality standards?
B. Ask for evidence of the benefits of OPD as opposed to MDS.
C. Ask for evidence to back up the claim that OPD will help reduce polypharmacy? (In my view this is a bizarre claim).
D. Ask for evidence to back up the claim that OPD will reduce medicines waste.
E. Ask the residents or their families, or (if there’s a Lasting Power of Attorney [LPA] or Court of Protection order in place), ask the Attorneys or Deputys.
F. Ask the staff.
G. Ask the prescribers.
I’m interested in feedback on this. I am a nurse by trade and used to be a proponent of OPD in all circumstances. Since working in social care and with residential homes I’ve re-visited this view.
Care home residents need well designed systems. Unless the patient can manage their medicines themselves (always the first consideration), a good MDS system is often a safer way to administer medicines.
4.2 . The benefits of using electronic MAR charts.

These fall into three categories.
- Improved legibility.
- Improved access (e.g., if the charts are accessed and updated on a computer or portable device there is less risk of losing, damaging, or mislaying them).
- eMAR chart systems that obtain the data taken directly from the Community Pharmacy system eliminate the need for transcribing, which is a high-risk area.
In addition to the three benefits mentioned, carefully planned, and implemented eMAR systems contribute to a decrease in medicines errors, reduced administrative costs and improved quality of care.
Click here to read more about eMAR systems.

Last updated: 06.10.2024
Useful links:
NICE Guideline Managing Medicines in Care Homes
NICE Quality Standard Managing Medicines in Care Homes
CQC Managing Medicines in Health and Adult Social Care
