Medicines optimisation in long-term pain.
‘#jargonbuster ‘Medicines Optimisation’ means getting the medicines right for the individual. This may involve an alternative medicine, an alternative treatment or approach, and / or not taking medicines. The person’s experience, beliefs and what matters to them most should drive this decision, with clinicians providing guidance, advice and education on trusted sources of information, the evidence base and on safety’. (Steve Turner)
This is a brief summary relating to a topic in the 2018 update of Medicines optimisation: key therapeutic topics
To access the pain management topic [KTT21] click here.
The section on medicines optimisation in long term pain contains a huge amount of information, including links to numerous other documents, on an areas critical to patient safety & wellbeing.
Key points:
- There is little evidence that opioids are helpful for long-term pain.
- Patient safety incidents relating to the unsafe doses of opiates remain a major concern. People develop a ‘tolerance’ to opiate medicines, meaning that higher and higher doses may be needed to deliver the same effect. However this tolerance rapidly goes away when the opiates are stopped, so restarting at the old dose may be fatal.
This image is taken from: ‘Opioids Aware: A resource for patients and healthcare professionals to support prescribing of opioid medicines for pain.
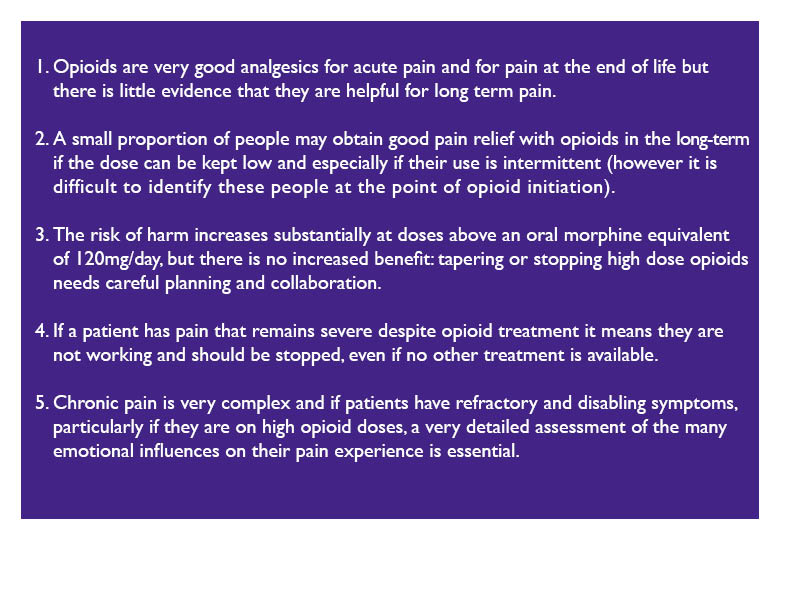
Click on the image to enlarge it.
Link: http://www.rcoa.ac.uk/faculty-of-pain-medicine/opioids-aware
‘A review of medicines-related safety incidents involving controlled drugs reported to the NRLS over 7 years found the risk of death with controlled drug incidents was significantly greater than with medication incidents generally (odds ratio 1.48, 95% CI 1.02 to 2.17). Incidents involving overdose of controlled drugs accounted for 89 (70%) of the 128 incidents reporting death or severe harm. Five controlled drugs (morphine, diamorphine, fentanyl, midazolam and oxycodone) were responsible for 113 (88%) of these 128 incidents.’
Non-opioid medicines in long-term pain
- Patients can be prescribed gabapentin or pregabalin for certain types of pain. Both of these medicines can lead to dependence and may be misused or diverted.
#jargonbuster ‘diverted’ = passed on or sold one to someone else.
Finally, emotional influences are real:
-
When assessing pain with someone it’s vital that clinicians take all aspects of the person’s life into account, including lifestyle, nutrition, hydration, social and housing factors, safeguarding, sleep and rest, other illnesses, emotional influences and their mental health.
And take a full history of medicines being taken, or recently stopped, including over the counter medicines, internet bought medicines, borrowed medicines and illicit substances.
Overall key points to remember on pain management:
-
Adopt a holistic patient-centered approach
-
Aim to prevent acute pain becoming chronic pain
-
There is little evidence that opioids are helpful for long-term pain
Related Guidance:
NICE Guidance NG5 Medicines Optimisation
NICE Guidance NG59 Low back pain and sciatica in over 16s: assessment and management
NICE Guideline NG46 Controlled drugs safe use and management
NICE Guidance CG140 Palliative care for adults: strong opioids for pain relief
Steve is a nurse prescriber, Head of Medicines and Prescribing for @MedicineGov , Associate Lecturer at Plymouth University and NICE Medicines and Prescribing Programme Associate.

Author: Steve Turner
First published 1/8/2017. Revised and updated 13/12/2018
